Or do they buy less healthy food and stick with the junk?
Genuine question.
Wegovy surely just removes appetite and people will still desire the food that they crave more than the food which they don’t, but which may be healthy.
Or do they buy less healthy food and stick with the junk?
Genuine question.
Wegovy surely just removes appetite and people will still desire the food that they crave more than the food which they don’t, but which may be healthy.
Well, if they buy junk food they will be less inclined to eat it all. That Giant Economy size packet of crisps may take 2 or 4 days to consume.
I think we can be fairly confident that Nestlé et all are paying attention.
From experience, Wegovy et al slow the emptying of the digestive tract. This works for heavy and fatty meals (like burgers and fries), but doesn’t work so well against sweets. So Nestle isn’t likely to be harmed a great deal.
Good vid, like Jeff Nippard, been watching him for years for weightlifting. BMI is a very blunt metric and contains no useful information.
On weight loss, I am waiting to hear from my Dr if insurance will cover Mounjaro, decided to give the GLP1-RAs a go. Historically always struggled with weight, only thing that worked for me was going to a nutritionist who ACTUALLY listened to me and produced a tailored food schedule. Most of them don’t listen and just throw out some bullshit 1980s programme with 6 slices of bread per day, 8 micromeals “to keep your metabolism running”, and of course everything tastes like boiled sponge because all fat is eliminated.
I believe it is quite a lot of time and money to get GLP1 approval via insurance. Wegovy costs me around 180chf a month, which is probably negated by buying less crap food. This also gives me the incentive to one day ween off it.
Here in the Fatherland it is not covered.
I asken my doc about it and was advised that it is damaging to the liver, something I can’t afford.
He sent me to a nutritionist and I got the same 1980ties crap you mention along with a side order of secret “magic powders” patentid by a Dr. Whoever for 4000€
I asked what it contained… “its a secret”
“How can it be a secret if it is patented” I asked.
I let her squirm for a few minutes before leaving.
@Slammer I assume you mean Germany? If so then yes - I’m in healthcare myself and know Germany considers some conditions as “lifestyle” and does not reimburse (erectile dysfunction, obesity, alopecia, vitiligo come to mind). What they probably miss that Switzerland is not missing is how much it costs to treat diabetes, stroke, infarctions, the loss of life, disability and productivity losses they lead to. Switzerland is smarter in this in my opinion, choosing to pay a bit now and save a ton later.
Why is that? The Dr told me Wegovy is about 180/month if out of pocket, and Mounjaro is about 380/month. Indeed, I had my appt about 6 weeks ago and haven’t heard back.
However, the Dr also told me that the only intervention that has robust long-term data for long-term weight loss is…gastric bypass, and that that’d be their recommendation given my age and circumstance. The thing is, I said I see this as a major injury to an otherwise healthy body and organ. Yes, obesity is a condition, and leads to several serious conditions that cost tens/hundreds of thousands (diabetes, infarctions, stroke) so in a way I can say my body is not healthy, however getting surgery is something that’d mess up my weightlifting, I’d worry if the sutures would hold long term. If it was cancer (touch wood) I’d tell the Dr “take the bastard out today”, but doing plumbing in my plumbing is not something I want.
This was my point above. The impacts of GLP-1 treatment seems to broad and beneficial that healthcare systems might actually save money by paying to provide it now and avoid more expensive care/treatment later. An ounce of prevention worth a pound of cure and all that…
Yes, but that ounce costs more than an ounce of gold. And the jury is still out on whether these are forever drugs.
They’ve gone generic in a few countries so should become cheaper.
I lift weights, cycle, swim, swing my mace bells and do kettlebells that much I can crack wallnuts between my ass cheeks, I watch what I eat and what I drink.
I was advised by the doc to visit a surgeon, which I did…
I collected data on my food intake for over six weeks ready to present.
The doc looked at me and immediately said “Schlauchmagen” meaning taking out the entire stomach.
He did not even glance at my data.
Not going to happen because as you say I dont want bits removed.
The Dr who saw me said that gastric sleeve is “not preferred”…
Interestingly, my Dr asked me why I said no - I said it’s not philosophical, ethical or religious, it’s just that I don’t want to have as drastic a thing done to my body for what I consider not a good enough reason. In some ways I even consider it an easy way out, you go to sleep, wake up and are physically unable to eat much. They said “For you it’d make sense, when I see 18 year old kids at 150kg I tell them they need to try other ways first”. Incidentally gastric bypass would turn out cheaper for both me and the insurance, I feel!
Yep, all the patent cliffs scaring pharma nowadays will turn out to be very good for patients, a myriad of phenomenally good drugs have come out the last 15-20 years which are now too expensive but will soon be readily available everywhere.
And they are right.
The percentage of patients who regain their original weight after gastric bypass surgery is less than 5%.
For Wegovy, for those who come off it, on average, patients regain about two-thirds (60% to 75%) of the weight they originally lost within the first year of stopping the medication. Around 50% regain most of their original weight.
Currently, with a 50% change of regaining the weight suggests these are a forever-drug.
That’s the issue. Until some years pass and more data is collected, we’re stuck in the “seems to be beneficial”. Making broad decisions based on “seems” is reckless. Specially when the situation is not an emergency (on average).
From the cautuin side, what is good for an individual is not necessarily good for a population.
There must be a reasonable chunk of data to plug in (20 years or so?), given that some of these therapies have already been used for years in diabetics. Side effects are side effects regardless of what the use of the drug is, right?
It’s obviously beneficial - it works for weight loss but for many, the weight comes on if the drug is stopped.
There’s the danger that if this becomes a freely-available, low cost treatment then future generations will have no need to “watch-their-weight” and will eat what they want knowing there is a simple, pain-free solution.
One of the biggest problems I see is that it doesn’t stop people eating unhealthily and quantity of food is only one part of the equation.
Do people on the drug start eating more salads, beans, Low G.I. carbs like oats instead of the unhealthy diet which made them obese in the first place or do they continue as they were, but with smaller quantities.
There’s so much mis-information spread about diet and food in the media, social or otherwise - and even on this forum that even if people try and eat healthily, so many are going to get it unintentionally wrong.
Are we going to end up with a population predominately made up of thin, incredibly unhealthy people rather than obese, unhealthy people?
Yes, But.
They are used to either avoid people at risk from developing T2 diabetes or to help those who already have the disease with managing their blood glucose levels. It is not a treatment for TYPE ONE. Dramatic weight loss in these patients can be problematic and the dosages are moderated because of this. But these treatments are forever treatments and the dramatic surge in demand for GPLs, and significant cost increases are putting them out of reach for many T2s.
Yes, I get all of that but my point was that there is a solid 20 years of widespread use which can provide a LOT of data - good, bad and indifferent, which is what the original post was addressing.
I’ve read that it can be attributed to unexpected effects such as controlling addictive behaviour not only around food but also smoking, alcohol and even gambling, and the therapy itself can benefit vascular health (not entirely down to the patient managing their weight but as a direct result). There is also a suggestion that it can stave off neurological disorders such as Alzeimers or Parkinson’s Diseases.
All of this research would require many years of follow-up over a broad spectrum of the population.
I only know two people who take Mounjaro but they were both really desperate to lose weight and did overhaul their habits as well as start using the jabs.
In Switzerland at least the costs are reimbursed by the basic insurance if they are used to treat diabetes. There are certain criteria to be met I believe but the T2 diabetics who would really benefit from it do get it reimbursed. I have a friend who uses ozempic to treat her T2 diabetes which is covered by the insurance and she has lost some weight as a bonus.
Thanks, I just learned these drugs are not something from 3-4 years ago.
Now, I’m curious. Actuaries at insurance companies are crunching the numbers. We all pay the same rate here in Switzerland, but the implication here is that taking the drugs may not be a free choice in other countries where insurance is priced individually. It’s a bit abstract (because insurers wrote it), but GLP-1s are a hazard of leaving money on the table due to under or overestimating risk, and that’s unacceptable. I guess we-ll get news soon about a 10% discount if the customer agrees to follow GLP-1s treatment and sticks to it.
Emerging evidence on the mortality impacts of GLP-1 drugs for both diabetics and non-diabetics presents opportunities to incorporate this data into underwriting risk assessments. Failing to account for GLP-1s – or including them without considering their nuanced benefit-risk profile – could place underwriting programs at a competitive disadvantage.
- Overestimation of risk: Programs may overestimate the risk in individuals experiencing lower mortality due to these treatments, leading to less competitive offers and a potential worsening of the metabolic risk pool.
- Underestimation of risk: Conversely, they may underestimate the risk in some individuals taking GLP-1s, where varied responses to treatment may lead to diverging outcomes.
- Loss of profitable business: The benefits to underwriting programs extend beyond improved ratings for those currently qualifying at substandard rates. These effects may also expand insurability for individuals currently viewed as uninsurable. Programs that ignore the impact of GLP-1s risk missing out on growth opportunities in this area.
As GLP-1s continue to reshape the landscape of obesity treatment and influence trends in long-term mortality, the ability to accurately assess metabolic risk has never been more critical. Carriers that choose to ignore this shifting landscape in their underwriting programs stand to lose out and may put themselves at a competitive disadvantage. Intelligent program design, making use of EHRs, offers a transformative opportunity to integrate robust longitudinal clinical data into risk assessment.
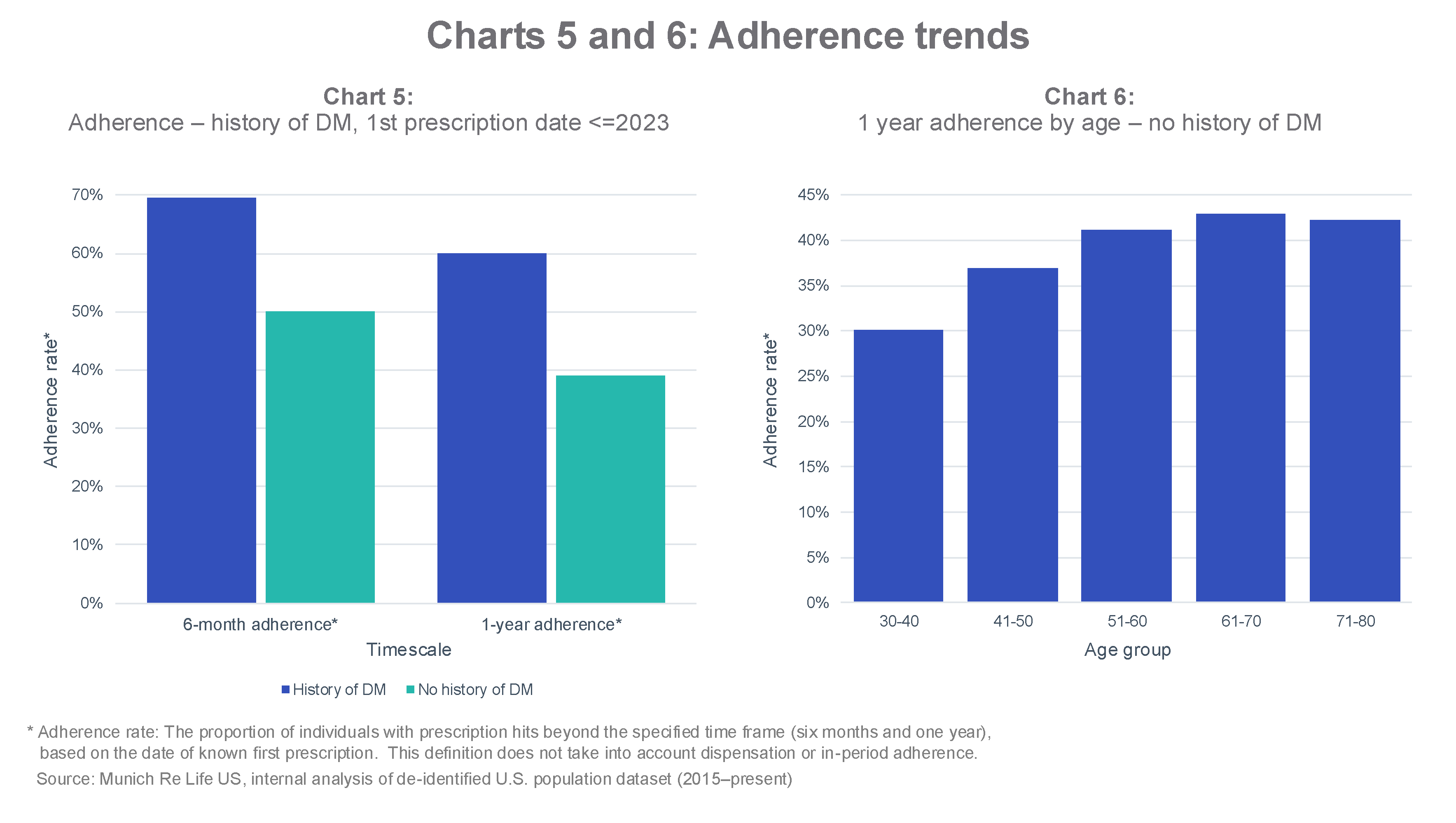
Side effects seem to be considerable, either to personal health or bank account. Only 60% of people with diabetes (DM) sticks to the treatment 1 year after the first prescription. For people with no DM, it’s only 40%. So, there’s a drug that can help people, great! But people don’t keep taking it. When looking at the adherence rate by age for people with no DM, it becomes clear it’s a lifestyle choice for the 31-40 YO. They just take it to attain a weight target, then bye bye.